Ethicon Womens Health & Urology
GYNECARE THERMACHOICE System
THERMACHOICE III Instructions for Use Aug 2010
Instructions for Use
20 Pages
Preview
Page 1
INSTRUCTIONS FOR USE GYNECARE® THERMACHOICE® III Uterine Balloon Therapy System Thermal Balloon Ablation Silicone Catheter and Syringe (Single-Use) Read all directions, precautions, and warnings prior to use. This instructions for use provides directions for using the GYNECARE® THERMACHOICE® III Uterine Balloon Therapy (UBT) System. CAUTION Federal law (USA) restricts this device to sale by or on the order of a physician with appropriate training.
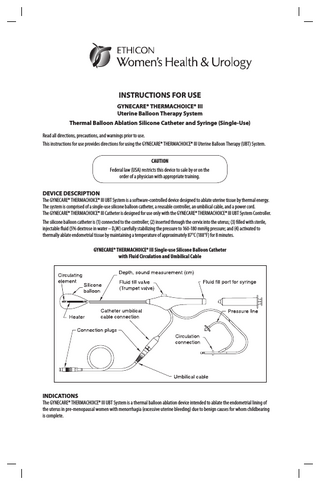
DEVICE DESCRIPTION The GYNECARE® THERMACHOICE® III UBT System is a software-controlled device designed to ablate uterine tissue by thermal energy. The system is comprised of a single-use silicone balloon catheter, a reusable controller, an umbilical cable, and a power cord. The GYNECARE® THERMACHOICE® III Catheter is designed for use only with the GYNECARE® THERMACHOICE® III UBT System Controller. The silicone balloon catheter is (1) connected to the controller; (2) inserted through the cervix into the uterus; (3) filled with sterile, injectable fluid (5% dextrose in water – D5W) carefully stabilizing the pressure to 160-180 mmHg pressure; and (4) activated to thermally ablate endometrial tissue by maintaining a temperature of approximately 87°C (188°F) for 8 minutes. GYNECARE® THERMACHOICE® III Single-use Silicone Balloon Catheter with Fluid Circulation and Umbilical Cable
INDICATIONS The GYNECARE® THERMACHOICE® III UBT System is a thermal balloon ablation device intended to ablate the endometrial lining of the uterus in pre‑menopausal women with menorrhagia (excessive uterine bleeding) due to benign causes for whom childbearing is complete.
CONTRAINDICATIONS The device is contraindicated for use in: • A patient who is pregnant or who wants to become pregnant in the future. Pregnancies following ablation can be dangerous for both mother and fetus. • A patient with known or suspected endometrial carcinoma (uterine cancer) or pre‑malignant change of the endometrium, such as unresolved adenomatous hyperplasia. • A patient with any anatomic condition (e.g., history of previous classical cesarean sections or transmural myomectomy) or pathologic condition (e.g., chronic immunosuppressive therapy) that could lead to weakening of the myometrium. • A patient with active genital or urinary tract infection at the time of procedure (e.g., cervicitis, vaginitis, endometritis, salpingitis, or cystitis) or with active pelvic inflammatory disease (PID). • A patient with an intrauterine device (IUD) currently in place.
WARNINGS Failure to follow all instructions or to heed any warnings or precautions could result in serious patient injury. General • The device is intended for use only in women who do not desire to bear children because the likelihood of pregnancy is significantly decreased following this procedure. There have been reports of women becoming pregnant following this procedure. Pregnancies after ablation can be dangerous for both mother and fetus. • Endometrial ablation using the GYNECARE® THERMACHOICE® III UBT System is not a sterilization procedure. The patient should be advised of appropriate birth control methods. • Patients who undergo endometrial ablation procedures who have previously undergone tubal ligation are at increased risk of developing post-ablation-tubal sterilization syndrome, which can require hysterectomy. This can occur as late as 10 years post‑procedure. • Endometrial ablation procedures using the GYNECARE® THERMACHOICE® III UBT System should be performed only by medical professionals who have experience in performing procedures within the uterine cavity, such as IUD insertion or dilation and curettage (D&C), and who have adequate training and familiarity with the GYNECARE® THERMACHOICE® III UBT System. • Endometrial ablation procedures do not eliminate the potential for endometrial hyperplasia or adenocarcinoma of the endometrium and may mask the physician’s ability to detect or make a diagnosis of such pathology. • DO NOT perform same-day GYNECARE® THERMACHOICE® procedure and hysteroscopic tubal occlusion/sterilization. Ablation may cause intrauterine synechiae, which can compromise (i.e., prevent) the 3-month confirmation test (HSG) for the tubal occlusion device. Women who have inadequate 3-month confirmation tests cannot rely on the tubal occlusion device for contraception. • Bench and clinical studies have been conducted which demonstrate that the GYNECARE® THERMACHOICE® procedure can be safely and effectively performed with nickel titanium tubal micro-inserts in place. However, the Thermachoice procedure should only be performed after the 3-month tubal occlusion confirmation test. Uterine Perforation • Uterine perforation can occur during any procedure in which the uterus is instrumented. Use caution not to perforate the uterine wall when sounding the uterus, dilating the cervix, or inserting the catheter. • Any of the following indicates possible uterine perforation: 1. If the catheter can be inserted to a greater depth than was determined by the uterine sound. 2. If the pressure cannot be stabilized at 160-180 mmHg with up to 35 mL of fluid (35 cc of fluid in the GYNECARE® THERMACHOICE® III device is approximately equal to the 30 cc used in the GYNECARE® THERMACHOICE® I clinical study), and there is no evidence of a balloon leak. 3. If the pressure drops precipitously at any point during the procedure. • If uterine perforation is suspected, THE PROCEDURE SHOULD BE TERMINATED IMMEDIATELY. • For patients in whom the procedure was aborted due to a suspected uterine wall perforation, a work-up for perforation should be considered prior to discharge. If a perforation is present, and the procedure is not terminated, thermal injury to adjacent tissue may occur if the heater is activated.
2
Technical • The GYNECARE® THERMACHOICE® III Balloon Catheter is for single use only – do not reuse or resterilize. • Do not treat patients for more than one therapy cycle in a given treatment session because of the potential for transmural injury to the uterus or injury to adjacent viscera. • Hold the catheter so it does not rest on the vaginal wall during treatment and cool-down periods to prevent possible burns. • Allow the catheter to complete the cool-down cycle prior to removal of the fluid. Remove the fluid and then the catheter. • After completing the procedure, it is important not to touch the GYNECARE® THERMACHOICE® III Balloon for the following reasons: – The balloon is covered with blood and body fluids. – There are mechanical and electrical parts that could puncture the balloon. • Proper care should be taken in disposing of the catheter.
PRECAUTIONS • The GYNECARE® THERMACHOICE® III UBT catheter, controller, and umbilical cable are designed as a system. To ensure proper function, never use other components with the GYNECARE® THERMACHOICE® UBT System. • A starting pressure of 160-180 mmHg is recommended and typically requires 6-15 cc of fluid and may require as much as 35 cc. Titration to achieve a stable pressure (no fluctuations greater than ±10 mmHg for at least 30 seconds) prior to activating the heating element is critical to proper functioning of the device. When inserting fluid, do not exceed a pressure of 200 mmHg. Typically, pressure levels decline slowly during the course of the procedure as the uterus relaxes. If a pressure of 160-180 mmHg cannot be reached with up to 35 cc or less of fluid, or if there is a rapid drop in pressure, it is likely there is a uterine perforation. • Rapid loss of pressure during a therapy cycle may indicate a uterine wall defect. Adding additional fluid to the balloon may create (or exacerbate if already present) a uterine wall defect such as a perforation. • Never add additional fluid during a therapy cycle. • Those patients who have undergone endometrial ablation and are later placed on hormone replacement therapy should have progestin included in their regimen in order to avoid the increased risk of endometrial adenocarcinoma associated with unopposed estrogen replacement therapy. • The safety and effectiveness of the GYNECARE® THERMACHOICE® III UBT System has not been fully evaluated in patients: – with submucosal myomas – with bicornuate or septate uteri or previous endometrial resection/ablation – with large uterine cavities (>35 cc in volume or uterine sound >10 cm) – with small uterine cavities (<2 cc in volume or uterine sound <6 cm) – undergoing repeat endometrial ablation procedures – who are post-menopausal • It has been reported that patients with a severe anteverted, retroflexed, or laterally displaced uterus are at an increased risk of uterine wall perforation during any intrauterine manipulation. The clinician should use discretion in patient selection. • A false passage can occur during any procedure in which the uterus is instrumented, especially in cases of severe anteverted, retroflexed, or a laterally displaced uterus. Use caution to insure that the device is properly positioned in the uterine cavity. • History of repeat low transverse Cesarean section may increase the risk of patient injury due to thinning of the myometrium.
3
ADVERSE EVENTS In a study of 134 women, performed with a previous-generation balloon catheter (version 1.2) [without the fluid circulation mechanism inside the balloon], the most frequent events reported during or after the procedure included: • Cramping/pelvic pain – Post-treatment cramping was reported in 91.8% of the patients. The cramps/pain ranged from mild to severe as reported during the intra-operative and immediate post-operative period. This cramping typically lasted a few hours and rarely continued beyond the first day following ablation. The use of non-steroidal anti-inflammatory drugs (NSAIDs) prior to and following GYNECARE® THERMACHOICE® UBT is usually sufficient to manage cramping and pelvic pain. • Nausea and vomiting – Nausea and vomiting were reported in 23.9% of the patients in the immediate hours following the procedure. This may be attributed to general anesthesia and was usually managed with medication. • Endometritis was reported in 2.1% of patients. All patients responded to a course of oral antibiotics. • Post-procedure symptoms such as pain, fever, nausea, vomiting, and difficulty with defecation or micturition were reported. Failure of such symptoms to resolve over a reasonable period of time warrants evaluation by appropriate medical personnel. • Pregnancy was reported in one patient (0.8%), resulting in a 2-month-premature live infant. Pregnancy following endometrial ablation may be dangerous to both mother and fetus. • Hematometra was reported in 0.6% of patients treated in clinical studies conducted outside the United States. In all patients in this trial, the hematometra was resolved with insertion of a uterine sound; however, there have been reports of hysterectomy due to hematoma or hematosalpinx. • A single perforation of the uterus was reported in one controlled clinical study. In a multicenter study of 250 women, performed with GYNECARE® THERMACHOICE® III (version 3.0), in which patients were randomized to receive either treatment with GYNECARE® THERMACHOICE® III with an additional post-procedure curettage (PPC Group) or treatment with GYNECARE® THERMACHOICE® III alone (NPPC Group), the following adverse events were reported during the first one year of follow-up. These events may or may not be related to the procedure. Table 1a. Adverse Events: Day of Procedure†
†
Adverse Event
NPPC Group N=124
PPC Group N=126
Endometritis
3 (2.4%)
2 (1.6%)
Vaginal burn
0
2 (1.6%)
Other abdominal or pelvic pain/cramping
1 (0.8%)
1 (0.8%)
Uterine perforation
1 (0.8%)
0
Post-op nausea
0
1 (0.8%)
Endometrial polyp removal
0
1 (0.8%)
Injury to tongue (bitten)
1 (0.8%)
0
Swollen hand
1 (0.8%)
0
Knot on wrist
1 (0.8%)
0
TOTAL
8 (6.5%)
7 (5.6%)
One subject in the NPPC Group experienced 3 adverse events
Table 1b. Adverse Events: ≥1 Day – 2 Weeks† NPPC Group N=124
PPC Group N=126
Bleeding or abdominal or back or pelvic pain/cramping
3 (2.4%)
2 (1.6%)
Discharge and/or vaginal infection
3 (2.4%)
2 (1.6%)
Endometritis
0
2 (1.6%)
UTI
0
1 (0.8%)
Fever
0
1 (0.8%)
Fainting
0
1 (0.8%)
Migraine headache
0
3 (2.4%)
Worsening carpal tunnel syndrome
0
2 (1.6%)
6 (4.8%)
14 (11.1%)
Adverse Event
TOTAL Three subjects in the PPC Group experienced multiple adverse events
†
4
Table 1c. Adverse Events: >2 Weeks – 1 Year†‡ Adverse Event
NPPC Group
PPC Group
Abdominal or back or pelvic pain/cramping
9 (7.3%)
8 (6.3%)
Discharge and/or vaginal infection
9 (7.3%)
6 (4.8%)
Bleeding
6 (4.8%)
4 (3.2%)
UTI or cystitis or urinary incontinence
5 (4.0%)
3 (2.4%)
Uterine fibroid or cervical polyp or vulva warty lesion removal
2 (1.6%)
1 (0.8%)
Abnormal Pap (ASCUS)
2 (1.6%)
0
Endometritis
1 (0.8%)
1 (0.8%)
Sinus congestion or infection or polyp
2 (1.6%)
5 (4.0%)
0
2 (1.6%)
1 (0.8%)
1 (0.8%)
Hot flush
0
1 (0.8%)
Hypothyroidism
0
1 (0.8%)
Depression
0
1 (0.8%)
Migraine headache
0
1 (0.8%)
Exacerbation of multiple sclerosis
0
1 (0.8%)
Cholecystolithiasis
0
1 (0.8%)
Hernia
1 (0.8%)
0
Bloody stool
1 (0.8%)
0
Cracked distal fibula
1 (0.8%)
0
Plantar fasciitis
1 (0.8%)
0
TOTAL
41 (33.1%)
37 (29.4%)
Ear infection or toothache Asthma or bronchitis
This table includes data from patients (5 NPPC, 3 PPC) who had their “12-month” visit at more than 1 year post-procedure. Note: There was one additional adverse event (pelvic pain) reported in the PPC Group, but the time interval was unknown. ‡ Six subjects in NPPC Group experienced multiple adverse events. Five subjects in PPC Group experienced multiple adverse events. †
OTHER ADVERSE EVENTS As with all endometrial ablation procedures, serious injury or death can occur. The following adverse events could occur or have been reported in association with the use of the GYNECARE® THERMACHOICE® III UBT System: 1. Rupture of the uterus 2. Thermal injury to adjacent tissue 3. Heated liquid escaping into the vascular spaces and/or cervix, vagina, fallopian tubes, and abdominal cavity 4. Electrical burn 5. Hemorrhage 6. Infection or sepsis 7. Perforation 8. Post-ablation-tubal sterilization syndrome – This is a complication following endometrial ablation in women who have also previously undergone tubal ligation. The pathophysiology of this condition is believed to be related to the regeneration of endometrium in the cornual areas of the uterus. Blood from these glands can flow back into the proximal fallopian tubes in cases where the lower uterine segment is extensively scarred. The proximal oviduct becomes filled with blood and fluid, causing symptoms similar to those of an ectopic pregnancy. 9. Vesico-uterine fistula formation 10. Complications leading to serious injury or death
5
CLINICAL STUDIES Two studies that have evaluated the safety and effectiveness of the GYNECARE® THERMACHOICE® UBT System in treating menorrhagia in pre‑menopausal women are presented in this labeling. The first was conducted in support of the initial product approval and was done using the first-generation balloon catheter, GYNECARE® THERMACHOICE® I UBT. In 2006, a more recent study completed a 12-month follow-up on subjects treated with the third-generation device, GYNECARE® THERMACHOICE® III UBT. Results from both studies are summarized below. GYNECARE® THERMACHOICE® I GYNECARE® THERMACHOICE® I was the first-generation device that was marketed from December 1997 through 1999. The GYNECARE® THERMACHOICE® III device has multiple design modifications compared with GYNECARE® THERMACHOICE® I, which is no longer manufactured. The pivotal clinical trial data for the GYNECARE® THERMACHOICE® I is still applicable to GYNECARE® THERMACHOICE® III, and the amenorrhea rate for the GYNECARE® THERMACHOICE® I pivotal trial served as the (historical) control for the primary endpoint in the clinical trial of GYNECARE® THERMACHOICE® III. The pivotal clinical trial conducted to support the original approval of GYNECARE® THERMACHOICE® I, which was completed in 1997, is summarized below: Conclusions: The GYNECARE® THERMACHOICE® I (version 1.2) [without the fluid circulation mechanism inside the balloon], at twelve, twenty‑four, and thirty-six months of follow-up, balloon ablation was demonstrated to be at least as safe (with fewer intra-operative complications and shorter procedure times) and as effective as hysteroscopic rollerball ablation in reducing menstrual bleeding to a clinically acceptable level in menorrhagic women who had completed their childbearing. Furthermore, statistically equivalent and significant reductions in patient-reported dysmenorrhea (mild, moderate, severe menstrual cramps), PMS symptoms (mild, moderate, severe common PMS symptoms), and overall impact of menses on lifestyle (scale of 1-10; 1=none, 10=severe) were experienced by both groups. Purpose: The use of balloon thermal ablation for the treatment of menorrhagia for benign causes in an anatomically normal uterine cavity was compared with rollerball electrosurgical endometrial ablation with regard to safety and effectiveness. The primary effectiveness measure was a validated diary scoring system (adapted from Higham JM, O’Brien PMS, Shaw RW. Assessment of menstrual blood loss using a pictorial chart. Br J Obstet Gynaecol. 1990;97:734-9). Success was defined as the reduction of excessive menstrual bleeding to normal flow or less. Secondary endpoints evaluated were overall percent decrease in diary scores and responses from a quality-of-life questionnaire. The endpoints for safety were based on the evaluation of adverse events associated with each procedure, including device-related complications, time of procedure, and type of anesthesia used. Methods: This randomized, prospective, multicenter clinical investigation using the previous-generation non-circulating balloon catheter was conducted at 14 sites using investigators highly experienced with hysteroscopic rollerball endometrial ablation. All patients were ≥30 years old, were pre-menopausal, and had completed childbearing. All had an anatomically normal uterine cavity ≥4 cm and ≤10 cm. Three months of documented menorrhagia for benign causes was a requirement for inclusion and was confirmed with an average diary score of at least 150 points. Endometrial biopsy and Pap smear were required to rule out pre-malignant or malignant cervical uterine disease. No endometrial-thinning medications could be used for three months prior to treatment, and all patients underwent a three-minute suction curettage just prior to suction treatment. Selection of anesthesia regimen was left to the individual investigators. Treatment success was defined as reduction of menses to a diary score less than or equal to 75, reflecting eumenorrhea. In the original Higham study, a diary score of 100 had 86% sensitivity and 81% specificity for true menorrhagia for benign causes as determined by chemical analysis of the saturated pads. Patient Population • 260 patients in Intent to Treat (134 GYNECARE® THERMACHOICE® I; 126 ROLLERBALL) – 1 aborted ROLLERBALL for uterine perforation – 2 aborted (1 GYNECARE® THERMACHOICE® I; 1 ROLLERBALL) for submucous fibroid – 2 aborted GYNECARE® THERMACHOICE® I for inability to maintain device pressure • 255 patients treated with test or control device (131 GYNECARE® THERMACHOICE® I; 124 ROLLERBALL) Baseline demographic, physical exam, and gynecological variables were statistically equivalent between the test and control groups with regard to age (GYNECARE® THERMACHOICE® I 40.2 years, ROLLERBALL 40.9 years), race, body mass index, mean baseline diary score (GYNECARE® THERMACHOICE® I 552.5, ROLLERBALL 570), and other criteria.
6
Table 2. Subject Withdrawals Subjects
GYNECARE® THERMACHOICE® I
ROLLERBALL
Entered into study (Intent to Treat Population)
134
126
Procedure aborted
3
2
Receiving complete treatment
131
124
For whom 12-month data not available: Hysterectomy Withdrew
6 2 1
Lost to follow-up
10 3 4 • 1 daughter’s death • 1 menorrhagia • 1 depression • 1 amenorrhea @ 3 mo. 3 • 1 amenorrhea @ 3 mo. • 1 6-mo. diary score 32 • 1 6-mo. diary score 77
3 • 1 diary score 14 • 1 amenorrhea @ 3 mo.
For whom 12-month data available
125
For whom 2-year data not available: Hysterectomy Lost to follow-up
114
3 2 1 • 1 yr. hypomenorrhea
For whom 2-year data available
9 6 3
122
For whom 3-year data not available: Repeat ablation Hysterectomy Lost to follow-up
105
8 1 4 2 • both hypomenorrhea @ 2 yr. 1
Withdrew For whom 3-year data available
5
114
100
RESULTS Effectiveness Table 3. Effectiveness Bleeding Rates shows the success rates for the Intent to Treat Group (134 GYNECARE® THERMACHOICE® I; 126 ROLLERBALL) as based on diary scores at the 1-year follow-up of 75 or less. Success at 24 and 36 months, based on telephone questionnaires, is defined as elimination of bleeding or reduction to light or normal flow. The worst-case scenario is presented whereby each of the discontinued patients (described in Table 2 for subject withdrawals) is counted as a “failure” for calculating the values listed in the table. Only the amenorrhea rate at 1 year is statistically significantly different between treatment groups (p≤0.05). Table 3. Effectiveness Bleeding Rates – Intention to Treat Population† GYNECARE® THERMACHOICE® I (n=134)
ROLLERBALL (n=126)
Months Post-Treatment
12a
24b
36b
12a
24b
36b
Number of Successful Patients
101
109
106
97
95
94
Study Success Rate
75.4%‡
81.3%‡
79.1%‡
77.0%‡
75.4%‡
74.6%‡
# of Patients with Amenorrhea (# of patients with diary scores = 0)
19
16
17
31
23
27
Amenorrhea Rate (% patients with diary scores = 0)
14.2%§
11.9%‡
12.7%‡
24.6%‡
18.2%‡
21.4%‡
Based on diary scores Based on telephone questionnaires † See Table 2 for subject withdrawals ‡ Not statistically significant (p>0.05) § Statistically significant (p≤0.05) a
b
7
Table 4. Effectiveness Quality of Life presents the Quality of Life Questionnaire responses for patients who responded at 12, 24, and 36 months. Patients discontinued prior to the visit (described in Table 2) were not included in the calculations. There were no statistically significant differences between groups. Table 4. Effectiveness Quality of Life† GYNECARE® THERMACHOICE® I
†
ROLLERBALL
Months post-ablation
12
24
36
12
24
36
# of patients who responded to quality of life questionnaire
125
122
114
114
105
100
% patients with anemia pre-treatment (HCT)
29.9%
N/A
N/A
29.7%
N/A
N/A
% patients with anemia post-treatment (HCT)
11.6%
N/A
N/A
10.6%
N/A
N/A
% satisfaction: very satisfied or satisfied
96.0%
95.9%
95.6%
98.2%
98.1%
97.0%
% patients with reduction in dysmenorrhea
70.4%
72.1%
73.7%
75.4%
75.2%
78.0%
% patients unable to work outside the home pre-treatment
39.7%
39.7%
39.7%
41.9%
41.9%
41.9%
% patients unable to work outside the home post-treatment
4.0%
0.8%
2.7%
2.7%
2.9%
1.0%
% patients reporting severe impact on life pre-treatment
70.3%
70.3%
70.3%
78.6%
78.6%
78.6%
% patients reporting severe impact on life post-treatment
3.2%
4.9%
1.8%
1.8%
1.0%
2.0%
See Table 2 for subject withdrawals
Safety Table 5. Safety shows there were no intra-operative adverse events and 4 post-operative adverse events in the GYNECARE® THERMACHOICE® UBT Group (n=134). In the Rollerball Group (n=126), there were 4 intra-operative adverse events and 3 adverse events in the immediate post-operative period. These differences were not statistically significant. The mean procedure time for the GYNECARE® THERMACHOICE® patients was statistically significantly less than for the ROLLERBALL patients. Table 5. Safety GYNECARE® THERMACHOICE® I (n=134)
ROLLERBALL (n=126)
Intra-operative adverse events
None (0%)
2 fluid overload 1 cervical laceration 1 uterine perforation (3.2%)
Post-operative adverse events
1 post-coital bleeding 3 endometritis 1 UTI (3.7%)†
1 endometritis 1 hematometra 1 PATSS1 (2.4%)†
Mean procedure time (minutes) Procedure time is duration between patient prep and catheter removal
27.4‡
39.6‡
PATSS = post-ablation-tubal sterilization syndrome Not statistically significant (p>0.05) ‡ Statistically significant (p≤0.05) 1 †
Anesthesia Regimen Selection of anesthesia regimen was left to the individual investigators. Fewer cases were performed under general anesthesia in the GYNECARE® THERMACHOICE® I Group as compared to the Rollerball Group. For GYNECARE® THERMACHOICE® I, only 53.7% had the procedure under general anesthesia (approximately 46% under local) versus 84.1% who had the Rollerball procedure performed using general anesthesia (approximately 16% under local).
8
Hysterectomy There were a total of 22 patients (8 GYNECARE® THERMACHOICE® I; 14 ROLLERBALL) who had hysterectomies within 3 years following endometrial ablation. Table 6. Hysterectomy Reason for Hysterectomy
Total† GYNECARE® THERMACHOICE® I (n=134)
ROLLERBALL (n=126)
Possible carcinoma (found negative)
0
1
Menorrhagia/abnormal bleeding
3
5
Pelvic pain/severe dysmenorrhea
4
6
Endometriosis/ovarian cysts
1
2
8 (8.6%)
14 (11.1%)
Total
†13 hysterectomies were in patients <40 years (4 GYNECARE® THERMACHOICE®, 9 ROLLERBALL); 9 hysterectomies were in patients >40 years (4 GYNECARE® THERMACHOICE®, 5 ROLLERBALL).
GYNECARE® THERMACHOICE® III GYNECARE® THERMACHOICE® III Catheter includes an active mechanism for circulation of the D5W within the balloon. Laboratory testing showed that the active circulation of fluid within the balloon will lead to a more even distribution of heat at the balloon surface, and thereby over the endometrial tissue. A clinical investigation was conducted to determine the incidence of post-procedure amenorrhea among women treated with GYNECARE® THERMACHOICE® III. Conclusions: In a study performed with GYNECARE® THERMACHOICE® III, the primary effectiveness analysis (ITT-matched subjects comparison between historical GYNECARE® THERMACHOICE® I data and GYNECARE® THERMACHOICE® III (GYNECARE® THERMACHOICE® III, NPPC Group only) evaluated amenorrhea at 12 months after ablation. Results revealed that 32.6% of women experienced amenorrhea at 12 months after ablation with GYNECARE® THERMACHOICE® III as compared to 13.7% after ablation with GYNECARE® THERMACHOICE® I. The difference in amenorrhea rates between these groups was statistically significant (p=0.0025). The observed rate of return to normal bleeding levels was greater in NPPC subjects treated with GYNECARE® THERMACHOICE® III compared to GYNECARE® THERMACHOICE® I (82% vs. 77%). This difference was not statistically significant. In the Intent to Treat analysis for all treated subjects comparing subjects receiving no post-procedure curettage (NPPC) to those receiving post‑procedure curettage (PPC), 37.1% (NPPC) and 33.3% (PPC), respectively, experienced amenorrhea at 12 months after ablation with GYNECARE® THERMACHOICE® III. There was no statistically significant difference in amenorrhea rates between NPPC Group and PPC Group (p=0.53). Similar rates of return to normal bleeding were observed in the NPPC Group compared to the PPC Group after GYNECARE® THERMACHOICE® III ablation. Therefore, given these results and the added risks associated with post-procedure curettage, this additional procedure is not recommended after ablation unless otherwise medically indicated. Purpose: The purpose of the GYNECARE® THERMACHOICE® III study was to determine the incidence of amenorrhea 12 months posttreatment among women treated with the GYNECARE® THERMACHOICE® III UBT System for the treatment of menorrhagia as compared to the incidence of amenorrhea observed in the original GYNECARE® THERMACHOICE® I UBT System clinical trial. There were additional secondary study objectives: • To confirm the post-procedure incidence of normal bleeding levels observed with GYNECARE® THERMACHOICE® III UBT System was comparable to the incidence of normal bleeding levels observed in the original GYNECARE® THERMACHOICE® I UBT System clinical trial • To determine the effect of a post-procedure curettage on bleeding patterns and post-operative discharge and post-operative pain • To evaluate changes in Quality of Life (QoL) following the procedure • To evaluate system usability Study Endpoints: For the primary objective, the incidence of amenorrhea among subjects randomized to no post-procedure curettage was compared to the incidence of amenorrhea among subjects who participated in the original GYNECARE® THERMACHOICE® I UBT System clinical trial. The primary effectiveness measure was a validated diary scoring system (adapted from Higham JM, O’Brien PMS, Shaw RW. Assessment of menstrual blood loss using a pictorial chart. Br J Obstet Gynaecol. 1990;97:734-9). Subject success was defined as a diary score of zero. Secondary endpoints evaluated were “return to normal bleeding” as indicated by a PBLAC score of 75 or less, responses from a quality-of-life questionnaire, and system usability. The endpoints for safety were based on the evaluation of adverse events associated with each procedure, including device-related complications and type of anesthesia used. Randomization was performed to accomplish a secondary objective of the study, the evaluation of the effect of post-procedure curettage on bleeding patterns, and the safety evaluation of post-operative discharge and pain parameters. 9
Methods: This was a randomized, historically controlled, multicenter, 2-arm evaluation conducted at 13 sites with 250 patients diagnosed with menorrhagia. Eligible subjects who had given consent were randomized to post-procedure curettage or to no post-procedure curettage. Menstrual diary scores were collected pre-treatment and at intervals out to 12 months post-procedure. All patients were to undergo a pre-procedure sharp or suction curettage immediately prior to the ablation to thin the endometrial lining. Study subjects will be followed for a total of 36 months post-procedure. Study subjects were required to meet the following patient selection criteria: Inclusion Criteria The subject needed: • • • • • • • •
to be a pre-menopausal female at least 30 years, in whom childbearing is complete excessive menstrual bleeding, documented by a diary score of at least 150 3 months of documented failed, refused, or contraindicated medical therapy an anatomically normal uterine cavity sounding at least 4 cm, but not greater than 12 cm a normal Pap smear and no unexplained abnormal Pap smears within 1 year of the procedure to agree not to switch from hormonal to non-hormonal contraception or vice versa during or just prior to the study to agree to use reliable contraception throughout the study to agree to participate in the study, including all study-related procedures and evaluations, and document this agreement by signing the informed consent document Exclusion Criteria The subject could not have: • • • • • • • • • •
an active pelvic inflammatory disease (PID) or recurrent chronic PID active genital or urinary tract infection at the time of the procedure history of malignancy of the reproductive system within 5 years of study entry history of malignancy of the endometrium, endometrial neoplasia, determined by endometrial biopsy taken within 6 months of study entry cavity-distorting myomas determined by pre-operative hysterogram, hysteroscopy, or transvaginal sonography within 6 months of the procedure previous endometrial ablation procedure previous uterine surgeries (such as full thickness myomectomy, subserosal myomectomy, uterine reconstruction, or any surgery in which thinning of the uterine musculature could occur) except for low transverse cesarean section been pregnant or desirous of future pregnancy taken endometrial suppression therapy, except for oral contraceptives, within 3 months of procedure concurrent open or laparoscopic surgery
Patient Population Patients were between the ages of 28 and 55, with 37.2% under the age of 40 (inclusive), and 62.8% over the age of 40 years. Baseline demographic, physical exam, and gynecological mean variables were not statistically different between the test and control groups with regard to age (NPPC 42 years, PPC 42.1 years), race, body mass index, and baseline diary score (NPPC 752.4, PPC 659). The following table (Table 7) describes the accountability of subjects throughout the study period.
10
Table 7. Subject Accountability SUBJECTS
NPPC
PPC
TOTAL
124
126
250
1
3
4
Receiving complete treatment
123
123
246
Details for patients with 12-month data not available: Hysterectomy Withdrew Lost to follow-up Unable to treat Incomplete data
4 3 10 1 0
4 3 9 3 2
8 6 19 4 2
For whom 12-month data is available
106
105
211
Details for patients with 24-month data not available: Hysterectomy Repeat endometrial ablation Withdrew Lost to follow-up Returned at 24 months
5 0 0 6 0
9 1 1 4 (+2)
14 1 1 10 (+2)
For whom 24-month data is available
95
92
187
Details for patients with 36-month data not available: Hysterectomy Repeat endometrial ablation Withdrew Lost to follow-up Returned at 36 months
3 0 2 3 (+3)
0 1 0 1 (+1)
3 1 2 4 (+4)
For whom 36-month data is available
90
91
181
Entered into study (Intent to Treat Population) Unable to treat
RESULTS Effectiveness – Bleeding Comparison to Historical Control Subjects from the original GYNECARE® THERMACHOICE® I study were matched to subjects from the GYNECARE® THERMACHOICE® III (NPPC subjects) study using the Propensity score method at 1 year post-procedure. This included an identification of the covariates affecting treatment difference between the GYNECARE® THERMACHOICE® III and GYNECARE® THERMACHOICE® I study, balancing the covariates using Propensity score method, and then analysis of the results using matched and unmatched data. The matched data were used to test the (null) hypothesis that the amenorrhea rates in GYNECARE® THERMACHOICE® I and GYNECARE® THERMACHOICE® III treated subjects at 1 year are the same. Results showed that the amenorrhea rate for subjects treated with GYNECARE® THERMACHOICE® III was significantly higher than the amenorrhea rate for the matched cohort from the GYNECARE® THERMACHOICE® I study (p=0.0025). These results are found in Table 8a. Table 8a. Effectiveness – Amenorrhea: GYNECARE® THERMACHOICE® III NPPC vs. GYNECARE® THERMACHOICE® I (Matched Subjects) at 1 Year Study Group Analysis Population
ITT Matched Subjects
GYNECARE® THERMACHOICE® III NPPC
GYNECARE® THERMACHOICE® I
% (# Successes/n)
32.6% (31/95)
13.7% (13/95)
95% C.I. for Success Rate
(23.4% - 43.0%)
(7.5% - 22.3%)
P value for GYNECARE® THERMACHOICE® III NPPC vs. GYNECARE® THERMACHOICE® I 0.0025
The post-procedure incidence of amenorrhea observed in all subjects treated with GYNECARE® THERMACHOICE® III (NPPC and PPC) was also compared to the incidence of amenorrhea observed in the original GYNECARE® THERMACHOICE® I Uterine Balloon Therapy System cohort at the cycle following the 1-, 2-, and 3-year post-ablation anniversary date. Amenorrhea was defined as a PBLAC score of 0 at 1 year and patient report of “amenorrhea” in response to a telephone interview, mailed questionnaire, or clinician visit at the 2- and 3-year time points. The results of the ITT analysis that considered missing data as failures showed that the amenorrhea rate 11
for subjects treated with GYNECARE® THERMACHOICE® III was significantly higher than the amenorrhea rate for subjects treated with GYNECARE® THERMACHOICE® I (one-tailed p=0.001 at 1 year, 2 years, and 3 years). These results are found in Table 8b. Table 8b. Effectiveness – Amenorrhea: GYNECARE® THERMACHOICE® III vs. GYNECARE® THERMACHOICE® I (All Subjects) ITT Population at 1, 2, and 3 Years† Study Group Time Point
12 months 24 months 36 months
GYNECARE® THERMACHOICE® III
GYNECARE® THERMACHOICE® I
% (#Successes/N)
35.2% (88/250)
14.5% (19/131)
95% C.I. for Success Rate (One-sided)
(30.2% - 100%)
(9.7% - 100%)
% (#Successes/N)
25.6% (64/250)
12.2% (16/131)
95% C.I. for Success Rate (One-sided)
(21.1% - 100%)
(7.8% - 100%)
% (#Successes/N)
26.8% (67/250)
13.0% (17/131)
95% C.I. for Success Rate (One-sided)
(22.2% - 100%)
(8.4% - 100%)
P value for GYNECARE® THERMACHOICE® III vs. GYNECARE® THERMACHOICE® I (one-tailed) <0.0001 0.001 0.001
Intent to Treat (ITT) population represents all subjects enrolled in the study, including those considered as failures because they were not available for follow-up. Therefore, the ITT Group represents a worst-case scenario for effectiveness. †
The effectiveness of GYNECARE® THERMACHOICE® III compared to GYNECARE® THERMACHOICE® I [matched subjects from GYNECARE® THERMACHOICE® III (NPPC) to GYNECARE® THERMACHOICE® I] was also evaluated in terms of achieving normal bleeding at one year post-procedure. This was defined as a PBLAC score of 75 or less. This information is provided in Table 9a, where subjects with missing data are considered failures. Table 9a. Effectiveness – Return to Normal Bleeding: GYNECARE® THERMACHOICE® III NPPC vs. GYNECARE® THERMACHOICE® I (Matched Subjects) at One Year ITT Effectiveness – Return to Normal Bleeding (Matched Subjects) % Return to Normal (#Successes/n)
Study Group GYNECARE® THERMACHOICE® III NPPC
GYNECARE® THERMACHOICE® I
82.1% (78/95)
76.8% (73/95)
P value for GYNECARE® THERMACHOICE® III NPPC vs. GYNECARE® THERMACHOICE® I 0.37
The effectiveness of GYNECARE® THERMACHOICE® III when compared to GYNECARE® THERMACHOICE® I in terms of achieving “normal bleeding” was evaluated in all subjects treated. Success at 1 year post-procedure was defined as a PBLAC score of 75 or less. Success at 2 and 3 years post-procedure was defined as a response of “normal,” “light,” “spotting,” or “amenorrhea” for GYNECARE® THERMACHOICE® III subjects and “eumenorrhea,” “hypomenorrhea,” “spotting,” or “amenorrhea” in GYNECARE® THERMACHOICE® I subjects. This analysis was based on the ITT population where missing data were considered as failures. At 1 year, the rate of return to normal bleeding was greater in GYNECARE® THERMACHOICE® III subjects (78.0%) than GYNECARE® THERMACHOICE® I subjects (77.1%). The difference in rates between the GYNECARE® THERMACHOICE® III and GYNECARE® THERMACHOICE® I Groups was not statistically significant (p=0.84). At 2 years, the rate of return to normal bleeding level or less was greater in GYNECARE® THERMACHOICE® I subjects (81.7%) than in GYNECARE® THERMACHOICE® III subjects (72.4%). The difference in rates between the GYNECARE® THERMACHOICE® III and GYNECARE® THERMACHOICE® I Groups was statistically significant (p=0.045). At 3 years, the rate was greater in GYNECARE® THERMACHOICE® I subjects (80.9%) than in GYNECARE® THERMACHOICE® III subjects (70.8%). The difference in rates between GYNECARE® THERMACHOICE® III and GYNECARE® THERMACHOICE® I Groups was statistically significant (p=0.03).
12
Table 9b. Effectiveness – Return to Normal Bleeding: GYNECARE® THERMACHOICE® III vs. GYNECARE® THERMACHOICE® I (All Subjects) ITT Population at 1, 2, and 3 Years† Study Group ITT Effectiveness – Return to Normal Bleeding
P value for GYNECARE® THERMACHOICE® III vs. GYNECARE® THERMACHOICE® I
GYNECARE® THERMACHOICE® III
GYNECARE® THERMACHOICE® I
% Return to Normal at 1 Year (#Successes/N)
78.0% (195/250)
77.1% (101/131)
0.84
% Return to Normal at 2 Years (#Successes/N)
72.4% (181/250)
81.7% (107/131)
0.045
% Return to Normal at 3 Years (#Successes/N)
70.8% (177/250)
80.9% (106/131)
0.03
Intent to Treat (ITT) population represents all subjects enrolled in the study, including those considered as failures because they were not available for follow-up. Therefore, the ITT Group represents a worst-case scenario for effectiveness. †
Randomized Cohorts An analysis was also conducted comparing amenorrhea rates for subjects receiving no post-procedure curettage (NPPC) to those receiving post‑procedure curettage (PPC) at 1 year after ablation with GYNECARE® THERMACHOICE® III. Table 10 shows the success rates for the Intent to Treat Group (124 NPPC; 126 PPC) as based on a reduction in diary score from ≥150 to zero at the 1-year follow-up visit. Each of the discontinued subjects (described in Table 7 for subject accountability) is counted as a “failure” for calculating the values listed in the table. There was no statistically significant difference between the amenorrhea rates of the NPPC and PPC Groups. Amenorrhea rates were also compared between NPPC and PPC Groups at 2 years and 3 years. For the Intent to Treat analysis with missing data considered failures, there was no statistically significant difference in amenorrhea rates between the NPPC Group and PPC Groups, both at 2 years (p=0.35) and at 3 years (p=0.28). Table 10. Effectiveness – Amenorrhea: GYNECARE® THERMACHOICE® III (NPPC vs. PPC) ITT Population at 1, 2, and 3 Years† Treatment Group GYNECARE® THERMACHOICE® III
Time Point
1 Year 2 Years 3 Years
NPPC
PPC
% (#Successes/N)
37.1% (46/124)
33.3% (42/126)
95% CI for Success Rate (One-sided)
(28.6% - 46.2%)
(25.2% - 42.3%)
% (#Successes/N)
28.2% (35/124)
23.0% (29/126)
95% CI for Success Rate (One-sided)
(21.6% - 100%)
(17.0% - 100%)
% (#Successes/N)
29.8% (37/124)
23.8% (30/126)
95% CI for Success Rate (One-sided)
(23.1% - 100%)
(17.7% - 100%)
P value for NPPC vs. PPC 0.53 0.35 0.28
Intent to Treat (ITT) population represents all subjects enrolled in the study, including those considered as failures because they were not available for follow-up. Therefore, the ITT Group represents a worst-case scenario for effectiveness. †
The effectiveness of GYNECARE® THERMACHOICE® III in the NPPC and PPC Groups was also evaluated in terms of achieving “normal bleeding.” Success at 1 year post-procedure was defined as a PBLAC score of 75 or less. Success at 2 and 3 years post-procedure was defined as a response of “normal,” “light,” “spotting,” or “amenorrhea.” This analysis was based on the ITT population where missing data were considered as failures. (See Table 11.) Table 11. Effectiveness – Return to Normal Bleeding: GYNECARE® THERMACHOICE® III (NPPC vs. PPC) ITT Population at 1, 2, and 3 Years† ITT Effectiveness – Return to Normal Bleeding
Treatment Group GYNECARE® THERMACHOICE® III
P value for NPPC vs. PPC
NPPC
PPC
% Return to Normal at 1 Year (#Successes/N)
80.6% (100/124)
76.2% (96/126)
0.39
% Return to Normal at 2 Years (#Successes/N)
73.4% (91/124)
72.2% (91/126)
0.84
% Return to Normal at 3 Years (#Successes/N)
71.0% (88/124)
70.6% (89/126)
0.95
Intent to Treat (ITT) population represents all subjects enrolled in the study, including those considered as failures because they were not available for follow-up. Therefore, the ITT Group represents a worst-case scenario for effectiveness. †
13
Effectiveness – Quality of Life Quality of Life (QoL) data was obtained using the same QoL questionnaire as was used in the GYNECARE® THERMACHOICE® I study. Patient satisfaction and improvement in some quality-of-life parameters at 12 months post-procedure are included in Table 12a. Results are provided based on the number of responders. There were no statistically significant differences between NPPC and PPC Groups. Table 12a. Effectiveness – Quality of Life NPPC
PPC
96.1% (99/103)
95.9% (94/98)
Percent of patients with reduction in dysmenorrhea
88.7% (94/106)
90.4% (94/104)
Patients who missed at least 1 day per month from work – PRE-TREATMENT
54.4% (49/90)
53.4% (47/88)
Patients who missed at least 1 day per month from work – 12 months POST-TREATMENT
1.3% (1/80)
2.7% (2/75)
Patients reporting severe impact on life score (8 to 10) – PRE-TREATMENT
74.0% (91/123)
75.2% (91/121)
3.9% (4/103)
9.1% (9/99)
Satisfaction: patients who were satisfied †
Patients reporting severe impact on life score (8 to 10) 12 months – POST-TREATMENT
†
12-month follow-up
†
At 2 years and 3 years, patients rated their satisfaction with treatment, indicating whether they were very satisfied, satisfied, or not at all satisfied. The results were comparable between NPPC and PPC both at 2 years and 3 years post-procedure. The results are presented in Table 12b. Table 12b. Effectiveness – Quality of Life: Patient Satisfaction with Treatment at 2 Years and 3 Years Time Point
NPPC
PPC
Satisfaction at 2 Years: Patients who were very satisfied Patients who were satisfied Patients who were not at all satisfied
84,2% (80/95) 11,6% (11/95) 4,2% (4/95)
82,8% (77/93) 15,1% (14/93) 2,2% (2/93)
Satisfaction at 3 Years: Patients who were very satisfied Patients who were satisfied Patients who were not at all satisfied
82,2% (74/90) 15,6% (14/90) 2,2% (2/90)
85,7% (78/91) 13,2% (12/91) 1,1% (1/91)
CLINICAL OBSERVATIONS Pre-Treatment Preparation for the Clinical Study All study subjects were supposed to undergo a pre-treatment suction or sharp curettage to thin the endometrium prior to ablation. However, due to investigator practice, not all subjects required curettage to thin the endometrium. An Intent to Treat analysis showed no significant impact of pre-treatment curettage on treatment outcome.
ANESTHESIA Anesthesia was delivered at the discretion of the investigator. The following table provides a summary of the types of anesthesia used in this study. Table 13. Anesthesia Use Group Types of Anesthesia
NPPC
PPC
Total
N
%
N
%
N
%
Cervical block only
5
4.03
1
0.79
6
2.40
Epidural only
0
0
1
0.79
1
0.40
General anesthesia only
77
62.10
80
63.49
157
62.80
Other anesthesia method only*
6
4.84
8
6.35
14
5.60
Cervical block and epidural
0
0
1
0.79
1
0.40
Cervical block and general anesthesia
17
13.71
14
11.11
31
12.40
Cervical block and other anesthesia method
18
14.52
20
15.87
38
15.20
General and other anesthesia method
1
0.81
0
0
1
0.40
Cervical block, epidural, and other anesthesia method
0
0
1
0.79
1
0.40
Total
124
100.00
126
100.00
250
100.00
NPPC, no post-procedure curettage; PPC, post-procedure curettage. *Other anesthesia methods included spinal, IV sedation, laryngeal mask airway (LMA), and monitored anesthesia care (MAC). 14
Hysterectomy Twenty-five subjects (12 NPPC; 13 PPC) had hysterectomies within 36 months following endometrial ablation. Table 14. Hysterectomy at or Before 36 Months Reason for Hysterectomy
Total* NPPC (n=12)
PPC (n=13)
Hyperplasia
0
1
Menorrhagia/abnormal bleeding
6
6
Menorrhagia/dysmenorrhea
3
1
Pelvic pain/severe dysmenorrhea
3
4
Fibroids
0
1
Total
12
13
*8 hysterectomies were in patients <40 years (2 NPPC, 6 PPC); 17 hysterectomies were in patients >40 years (10 NPPC, 7 PPC)
System Usability Summary System usability was evaluated on all 250 subjects undergoing treatment during this GYNECARE® THERMACHOICE® III trial. The System Usability endpoint was any case requiring an intervention to overcome a system issue after connection of the catheter to the controller has begun, i.e., having to restart. There were 28 cases of procedure events meeting this definition out of the 250 cases, resulting in a final rate of 11.2%. This rate demonstrates an improvement over that observed in the original GYNECARE® THERMACHOICE® I trial (18.6%) and in the GYNECARE® THERMACHOICE® II Post-Market Study (31.7%).
PATIENT SELECTION Menorrhagia can be caused by a variety of underlying problems including, but not limited to, endometrial cancer, myomas, polyps, anovulation, drugs, and dysfunctional uterine bleeding. Patients should always be evaluated to determine the cause of their excessive uterine bleeding before any treatment option is initiated. Consult medical literature relative to various endometrial ablation techniques, indications, contraindications, complications, and hazards prior to the performance of any endometrial ablation procedures. The patient selection criteria are: • Documented diagnosis of menorrhagia for benign causes • Completed childbearing • Pre-menopausal • Normal Pap smear and endometrial biopsy • Anatomically normal uterine cavity: standard sonography, saline infusion sonography, hysteroscopy, or hysterosalpingography within 6 months prior to performing GYNECARE® THERMACHOICE® UBT should be used to rule out submucous fibroids, large polyps, and congenital abnormalities • Uterine cavity depth of 6-10 cm • Failed or contraindicated medical therapy
PATIENT COUNSELING As with any procedure, the physician needs to discuss risks, benefits, and alternatives with the patient prior to performing endometrial ablation. In addition, the physician should discuss signs and symptoms of potential complications, such as bleeding, infection, or thermal injury. The device is intended for use only in women who do not desire to bear children because the likelihood of pregnancy is significantly decreased following this procedure. Post-procedure pregnancy may be dangerous for both mother and fetus. Patients of childbearing capacity should be counseled that endometrial ablation is not a sterilization procedure, and should be provided an appropriate birth control method. Patients of childbearing capacity should be cautioned of the potential complications which may ensue if they become pregnant. Vaginal discharge is typically experienced during the first few days following ablation and may last as long as a few weeks. Generally, the discharge is described as bloody during the first few days, serosanguinous by approximately one week, then profuse and watery thereafter.
SURGEON PREPARATION 1. Surgeon scrubs with antiseptic solution per local practice. 2. Surgeon dons sterile gown and sterile gloves per local practice.
SITE PREPARATION Anesthesia options include: • General • IV sedation and local • Local only • Regional (epidural, spinal) 15
Preparation Steps: 1. The patient is placed in the dorsal lithotomy position. 2. Surgeon thoroughly prepares perineum, vagina, and cervix with antiseptic solution per local practice. 3. The patient is draped, exposing perineum only. 4. A pelvic examination is performed to determine size, shape, and position of cervix and uterus. 5. The uterus is sounded. 6. Adequate visualization of the cervix is accomplished with appropriate speculum.
PRE-TREATMENT PREPARATION OF PATIENT The lining of the uterus should be thinned prior to GYNECARE® THERMACHOICE® III UBT. This can be accomplished by timing the menstrual cycle to the early proliferative phase, administering pre-treatment drugs such as danocrine or GnRH agonists, or performing suction or sharp curettage immediately prior to performing the endometrial ablation. The optimum pre-treatment regimens have not been determined at this time. It is recommended that a non-steroidal anti-inflammatory drug (NSAID) be given at least one hour prior to treatment and continued post-operatively as necessary to reduce intra-operative and post-operative uterine cramping.
DIRECTIONS FOR USE Please read all directions, precautions, and warnings prior to use. 1.0
SETUP
1.1
The following items are required for use of the GYNECARE® THERMACHOICE® III UBT System: GYNECARE® THERMACHOICE® III UBT System 1 sterile disposable GYNECARE® THERMACHOICE® III UBT silicone balloon catheter and syringe (30 cc) 1 umbilical cable 1 controller 1 power cord Medical Supplies 50 cc sterile injectable 5% dextrose in water (D5W) tenaculum, (weighted) speculum uterine sound, cervical dilator(s) sterile drape for umbilical cord (optional) Note: Use only plain D5W to inflate balloon catheter. Never use any other liquid. 1.2
Open the sterile package containing the GYNECARE® THERMACHOICE® III UBT Catheter and Syringe. Disinfect umbilical cable as described in the GYNECARE® THERMACHOICE® UBT System Operating Manual. Handle balloon portion of the catheter carefully to prevent damage.
1.3
Make sure that the controller power is off before making the connection (Steps 1.4–1.6).
1.4
Plug the power cord into the back of the controller and into the wall outlet.
1.5
The umbilical cable includes a connector plug at each end to connect the balloon catheter to the controller. Visually inspect the cable and connector plug to ensure there are no defects or signs of wear. Drape umbilical cable with sterile drape, if necessary, and attach the cable to the connector on the catheter (match arrows together). Attach the opposite end of the cable to the connection port on the front panel of controller. (Align red dots from umbilical cable to controller). (See Diagram 1) Note: When oriented correctly, the cable plugs will fit into the connectors easily and securely. Diagram 1
16
1.6
Connect the pressure line (pre-attached to balloon catheter) to the connection port (luer lock) on the front panel of the controller. Do not over-tighten, but ensure a snug connection or the device may not function properly. (See Diagram 1) Ensure that the pressure line is fully connected prior to adding any fluid to the system. Avoid loops, kinks, or bends in pressure line from controller to catheter to reduce the potential for motor fault issues. Periodically clean the entrance of the controller’s port, using a cotton swab with 70% isopropyl alcohol.
1.7
Remove the plug from the circulation catheter port. To remove the plug, press on the locking latch and pull the plug. Save the plug. It should be reinstalled when the controller is not in use. Connect the circulation catheter plug into the circulation port. It will lock into place with a slight click. Make sure it’s locked in by slightly pulling on it.
1.8
Turn on the controller power. The Message Display will read: Note: N.NN = software revision level
REVISION N.NN INITIALIZING
Message Display:
CONNECT CATHETER
Once catheter is connected, the Message Display will read:
PRIME CATHETER
The pressure line MUST be connected to the controller BEFORE the balloon catheter is filled with fluid, or the device will not function properly. 2.0 CATHETER PRIMING Note: When adding fluid during priming, ensure that the balloon fully opens so that none of its sides are touching. 2.1
FILL the 30 cc syringe with up to 20 cc (consistency w/2.4) of sterile injectable 5% dextrose in water (D5W). Use only sterile injectable 5% dextrose in water (D5W). Use of other fluids may compromise the system.
2.2
CONNECT the syringe to the port in the proximal end of the balloon catheter. Do not over-tighten syringe when connecting.
2.3
Point balloon catheter tip downward.
2.4
Press trumpet valve on top of balloon catheter handle and SLOWLY fill with up to 20 cc of D5W. Ensure that the pressure does not go above 200 mmHg (indicated by the pressure display on the controller).
2.5
Press trumpet valve and evacuate fluid and air from balloon to a negative pressure of –150 to –200 mmHg (indicated by pressure display on controller).
Note: You may need to purge air from the syringe several times to attain desired negative pressure. You must release the trumpet valve to maintain negative pressure. Air should be completely evacuated to optimize the function of the device. During priming, when catheter pressure is <–150 mmHg, the Message Display will read: PRIME CATHETER <–150 mmHg DO NOT EXCEED –200 mmHg negative pressure during evacuation. Excessive negative pressure can lead to greater pressure fluctuation during therapy.
2.6
The negative pressure creates a low-profile balloon insertion (balloon is drawn tight against catheter tip). Do not go beyond –200 mmHg. Check that negative pressure is maintained for at least 10 seconds before proceeding. Once catheter pressure is >–150 mmHg, the Message Display will read: INSERT CATHETER & FILL WITH D5W If negative pressure cannot be maintained for 10 seconds, remove the balloon catheter and replace. 3.0
PRESSURE TITRATION
3.1
Fill syringe to 30 cc with D5W, purge air, and connect to balloon catheter (do not over-tighten). Up to 5 cc of additional fluid may be used if needed, for a total of 35 cc.
3.2
Measure depth of uterus.
3.3
Using appropriate sterile technique and cervical/vaginal preparation, dilate cervix to 5 mm if necessary. If a perforation is suspected at this point, perform appropriate diagnostic measures to evaluate for perforation before proceeding. If perforation cannot be ruled out, abandon the procedure.
17
3.4
Wet the outside of balloon with D5W.
3.5
After sounding the uterus, and wetting the balloon, SLOWLY INSERT THE BALLOON CATHETER into the uterus until the tip is touching the fundus. Ensure that the depth indicated by markings on catheter is consistent with previous sound measurement. Use a tenaculum to hold the cervix if necessary.
3.6
Ensure that the cervix is dilated to 5 mm and do not use excessive force during insertion, as such force can cause the balloon to tear or the catheter to perforate the uterine wall. If a perforation is suspected at this point, perform appropriate diagnostic measures to evaluate for perforation before proceeding. If perforation cannot be ruled out, abandon the procedure.
3.7
Press trumpet valve on top of balloon catheter and fill balloon SLOWLY to pressure of 160-180 mmHg using 2-35 cc of D5W. (Release the trumpet valve to allow the pressure to stabilize.) Do not allow the pressure to exceed 200 mmHg during titration. Incrementally add small volumes to achieve a stable pressure (no fluctuations greater than ±10 mmHg) of 160-180 mmHg for a minimum of 30 seconds. The pressure of the balloon against the uterine wall often precipitates uterine contraction, thereby temporarily increasing the pressure reading. If pressure cannot be stabilized at 160-180 mmHg for 30-45 seconds with up to 35 cc of fluid, this may indicate uterine perforation. Remove the fluid and then remove the balloon catheter. If a balloon leak is present, replace the catheter and continue with the procedure. IF NO BALLOON LEAK IS FOUND, ABORT THE PROCEDURE. Note: Once the heater is activated, the pressure may initially rise 10-20 mmHg; the pressure may then drop slowly for the remainder of the procedure. The ending balloon pressure may be as low as approximately 100 mmHg and is typically between 120-150 mmHg. Note: It is recommended that for very small uteri, pressure titration should occur toward the lower end of the range (i.e., use a minimum amount of fluid to reach 160 mmHg. This will reduce the potential for increase of pressure during the thermal treatment that might result in over-pressure and system shutdown.) Note: Positioning the device in a false passage may allow the balloon to reach operating pressure with a small amount of fluid. This may be misinterpreted as being a small uterine cavity. Care should be taken to insure the device is properly positioned in the uterine cavity. Do not over-pressurize balloon during titration. Total fluid volume to achieve optimal balloon volume depends on the potential volume of the uterine cavity and is typically 6-20 cc at >160 mmHg (at start) and may be as great as 35 cc. If pressure level cannot be reached with up to 35 cc of fluid, remove balloon catheter and check for uterine perforation and/or balloon catheter leak. Replace balloon catheter if necessary.
4.0
TREATMENT
4.1 Message Display (alternating):
READY PRESS START
and
STABILIZE START PRESSURE >150 mmHg
When a steady pressure of 160-180 mmHg is maintained, press the START (
) button on controller to activate the heater.
Do not add fluid once heater is activated, as this could create (or exacerbate if already present) a uterine wall defect such as perforation. Hold the balloon catheter immobile and centered in the uterine cavity during procedure (with the valve oriented upward). Failure to hold the balloon catheter immobile during procedure can result in catheter failure. Warning: Ensure that the catheter is held such that it does not rest on the vaginal wall during treatment and cool-down periods to prevent possible burns. Note: Ensure that the balloon catheter is centered in the uterus to minimize potential overheat error codes during the treatment process. Prior to activating heater, ensure that fluid is on all sides of the catheter tip. It is no longer necessary to maintain contact with the fundus. 4.2
After the START button is pressed, the controller activates the heat to achieve the treatment temperature of 87°C (188°F) within 4 minutes. (This pre-heat cycle may take up to 4 minutes for larger uteri but is usually 15-45 seconds.)
PREHEATING TO 87°C
Note: If the treatment temperature of 87°C is not reached within 4 minutes, the controller will terminate the procedure. Remove the fluid and then remove the catheter. 18
Note: During treatment and in case of emergency, the STOP ( ) button can be pressed to terminate the procedure. The STOP button will power down the heater. The heater function can only be resumed by turning the unit off and restarting. 4.3
Message Display:
THERAPY CYCLE CYCLE 87°C, 8 MIN
Once 87°C is reached, an audible tone will indicate the automatic activation of the 8-minute therapy cycle. The time elapsed will be shown on the “THERAPY TIME” display. After the pre-heat cycle is completed, the time resets to 0:00. The displayed time represents the exact therapy cycle time. Note: Pressure may rise slightly with initial heating. It is common to then see the pressure fall gradually during procedure. If the pressure reaches 200 mmHg, an alarm will sound. If the pressure exceeds 210 mmHg for more than 2 seconds, the controller will terminate the procedure. The procedure may be restarted with a lower starting pressure to complete an 8-minute therapy. Note: A rapid drop in pressure or a failure to maintain pressure may be the result of a catheter leak or uterine perforation. After sufficient cooling, remove the fluid and then remove the balloon catheter and abort the procedure. A work-up for perforation should be considered prior to discharge. Note: Never add additional fluid during a therapy cycle as this could create (or exacerbate if already present) a uterine wall defect such as a perforation. 4.4
When the treatment cycle is completed, the Message Display will alternate between the following messages:
THERAPY COMPLETE
and
COOLING DOWN PLEASE WAIT
4.5
The controller automatically terminates the heater at the end of the treatment (cycle) and an audible alarm will sound.
5.0
POST-TREATMENT
5.1
The cool-down cycle takes 30 seconds. When the cycle is completed, the Message Display will read:
THERAPY & COOL DOWN COMPLETED
then
REMOVE FLUID REMOVE CATHETER
Remove fluid by drawing back on syringe while depressing trumpet valve. Remove all fluid from balloon. Remove the balloon catheter. Check that the entire fluid volume is withdrawn. 5.2
Disconnect the catheter pressure line from the controller.
5.3
Disconnect the circulation catheter plug from the controller.
5.4
Disconnect the umbilical cable from the catheter umbilical cable by pulling back on the gray collar.
5.5
Disconnect the umbilical cable from the controller by holding the stainless-steel ribbed shell and pulling back. Do not pull on the cable itself.
5.6
Discard the catheter. Retain the umbilical cable and disinfect for the next case.
5.7
The power must be turned off before beginning another procedure. Note: When a controller is left on without use for 8 hours, the controller freezes and displays the following message:
MAX TIME EXPIRED TURN POWER OFF
FOR ORDERING INFORMATION CALL: 1-800-255-2500 ORDERING INFORMATION AND RELATED PARTS AND ACCESSORIES REF #00825 #TC013 #TC003 #01105 #04995
DESCRIPTION GYNECARE® THERMACHOICE® UBT System Controller (Domestic) Sterile, single-use GYNECARE® THERMACHOICE® III (1-Pack) Sterile, single-use GYNECARE® THERMACHOICE® III Catheters (5-Pack) GYNECARE® THERMACHOICE® Umbilical Cable (reusable up to 20 applications) GYNECARE® THERMACHOICE® Power Cord (Domestic) 19
Manufactured by: ETHICON Women’s Health & Urology A Division of ETHICON, INC. Somerville, New Jersey 08876-0151 USA Tel: 1-877-384-4266
SYMBOLS USED ON LABELING
STERILE EO
Method of Sterilization- Ethylene Oxide Do not reuse/resterilize See instructions for use Batch number Use by-year and month
0086
CE Mark and Identification Number of Notified Body. Product conforms to the essential requirements of the Medical Devices Directive 93/42/EEC.
© Ethicon, Inc. 2010
389605.R07 LAB0011188.2 STATUS: 08/2010
389605.R07