Whip Mix
Accurad 200 Instruction Manual
Instruction Manual
36 Pages
Preview
Page 1
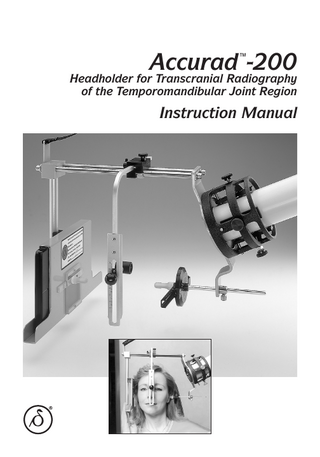
Accurad ™-200
Headholder for Transcranial Radiography of the Temporomandibular Joint Region
Instruction Manual
Acknowledgements It has been a gratifying experience to develop the Accurad™-200 headholder. This innovative instrument brings a new, broader dimension to transcranial TMJ radiography in order to meet the practitioner's everincreasing professional requirements. We wish to acknowledge the great contribution made by Dr. Bernard Williams to the development of the Accurad™-200 headholder. The "Twin Axis Adjustment Wheel" greatly expands the diagnostic capabilities of transcranial radiography by allowing doctors to adjust the angulation of the central X-ray beam to suit their individual needs and preferences for viewing each patient’s TMJ. It also allows precise quantification of patient head positioning and changes in the TMJ. Thanks also go to Drs. Terry Tanaka and Carl Rieder. Their experience and foresight were invaluable in taking the concept of the wheel and designing it for this instrument. We also wish to thank Dr. Harold Gelb for helping to bring transcranial TMJ radiography to the attention of dentistry. His efforts in educating the profession have helped many to understand the importance of this diagnostic modality. The evolution of the Accurad™-200 headholder also incorporates the invaluable suggestions made during the development stages by doctors including Al Crawford, Peter Dawson, Alvin Fillastre, Jack Haden, Yasuo Hatano, Charles Holt, Errol Lader, Hiroshi Muraoka, Gerald Murphy, Brendan Stack, Yoshitane Tanaka, George Tateno, Skip Truitt and John Witzig. We are very grateful for the suggestions and encouragement we have received while developing the Accurad™-200 headholder. This product embodies the technical sophistication needed to better serve modern dentistry.
1
The Accurad™-200 1. Horizontal Adjustment Scale 2. Support Strap 3. Anterior-Posterior Adjustment Scale 4. Beaded Support Chain 5. Film Transport Window with "SlideBar" to indicate Left and Right Sides 6. Fixed Ear Rod* 7. Nasion Piece* 8. Vertical Adjustment Scale
10
9. Film Cassette Transport 10. Film (to be purchased separately) 11. Patient Film Envelope 12. Film Cassette with Intensifying Screens 13. Allen Wrench 14. 12" and 16" Lead Aperture 15. Ruler
11
16. Adjustable Ear Rod* 17. Modified Twin Axis Adjustment Wheel 18. Universal Adapter Adjustment Knobs 19. Universal Adapter with Lead Aperture 20. Wall Chart (not shown) * Non-sterile. Disinfect before each use.
3
Actual Transcranial Radiograph
Maximum Open
Rest
Centric Occlusion
Maximum Open
Rest
Centric Occlusion
Landmarks to look for on the transcranial radiograph: Articular Eminence (A.E.) Mandibular Condyle (C.) External Auditory Meatus (E.A.M.) Glenoid Fossae (G.F.) Petrous Portion of Temporal Bone (P.T.B.) Petro-Tympanic Fissure (P.T.F.) 4
Table of Contents I Features and Benefits... 7 II Attaching the Accurad™-200 Headholder to the X-Ray Machine... 8 A. First -Time Attachment... 8 B. Selecting the Correct Lead Aperture... 9 C. Attaching Support Strap to Tubehead... 9 III Procedure for Use... 11 A. Loading the Cassette... B. Test Film Procedure... C. Test Film Troubleshooting... D. Patient Set-Up ... E. Adjusting the Nasion Aligner ... F. Recording Patient Positioning on the Film Envelope ... G. Exposing the Film... F. Radiographing the Temporomandibular Joint...
11 11 11 12 13 14 14 15
IV Appendices... 17 A. Clinical Specifications... B. Film Considerations... C. Troubleshooting... D. Procedure Variations... E. Anatomical Influences... F. Accurate Head Stabilization ... G. Manufacturer’s Notes...
17 17 19 20 25 25 26
V Exposure Charts... 27 1. Philips Oralix-65 Exposure Chart... 27 2. Lanex Rare Earth Intensifying Screens/OG Film... 28 3. Conversion Chart... 29 VI Warranty... 29 VII Care and Maintenance ... 29 VIII Bibliography ... 30
5
I. Features and Benefits With the increased emphasis on the treatment of occlusal and TMJ problems, there arose a need in the dental profession for a simple clinical instrument to obtain radiographs of the TMJ region. The Accurad™-200 headholder, incorporating the following features, meets and exceeds that basic need:
• Lead letters permanently affixed to "slidebar" over film transport window identify patient’s left and right TMJ directly on the film to aid in diagnosis and eliminate confusion. • Allows interchangeability between X-ray machines. • Six radiographs can be taken on one 5" x 7" film to provide a convenient means to evaluate TMJ relationships (mandible in maximum intercuspation, rest and maximum open positions). • Unit accommodates most patient head sizes. Lightweight plastic film cassette is easy to handle and store. • Color-coded indicator on film cassette minimizes confusion by identifying if the cassette is loaded/unloaded or if the film is exposed/ unexposed. • Sponge layer inside cassette ensures optimal film/screen contact. • Procedure can easily be delegated to auxiliary personnel.
• Attaches easily and securely to standard dental X-ray machines. • Used with the patient’s head in the upright position (norma lateralis) and with no head rest. This unstrained, natural vertical position avoids gravitational and unusual muscle influences induced by extreme postural positions of the head. • Accurate repeatability of patient positioning made possible by specially designed nasion aligner, ear rods for the external auditory meatus and fixed attachment to the X-ray machine. • The modified twin axis adjustment wheel allows for individualized transcranial TMJ radiographs. Adjustments on the modified wheel enable the horizontal and vertical angles of the beam to be changed allowing different views of the TMJ anatomy to appear on the radiograph for diagnosis and treatment.
7
II. Attaching the Accurad™-200 Headholder to the X-Ray Machine The Accurad™-200 headholder was designed to be used in conjunction with any standard dental X-ray machine. This instrument complies with applicable Department of Health, Education and Welfare standards under the Radiation Control for Health and Safety Act. In using this accessory instrument, be certain you proceed in accordance with the X-ray instructions provided by the manufacturer of your X-ray equipment. NOTE: Prior to installation and testing, all darkroom criteria must be met per instructions outlined in Appendix B.
Figure 2 3. First, adjust the clamp plates with red knobs. Position the ruler onto the adapter so the top right of the adapter frame seats into the square cut-out of the ruler with the shorter millimeter scale projecting towards the center of the round adapter opening (Figure 3). Center the ruler over the clamp plate to be adjusted. Turn the knob until the inner surface of the clamp plate aligns with the scale mark which corresponds to the cone dimension. Tighten until it is flush with cone adapter. This will allow you to quickly realign clamp plates should they become loose.
A. First-Time Attachment 1. Turn the four adjustment knobs of the cone adapter (Figure 1) to retract clamp plates to their maximum open position.
Figure 1 2. Measure the outer diameter of the X-ray cone with the millimeter scale (longer scale) of the supplied ruler (Figure 2). NOTE: Both height and width dimensions are required for rectangular cones.
Figure 3
8
4. To secure the X-ray cone, insert the cone into the adapter until it mates flush with the base of the lead cup and rests against the two preset clamp plates. While maintaining these contacts, turn the black knobs until the cone is securely held by the clamps (Figure 4).
G for comments regarding individual X-ray machines.
Figure 5
C. Attaching Support Strap to Tubehead
Figure 4
1. With the Accurad™-200 headholder attached to the cone, rest the cassette holder on a support (counter top, chair arm rest, etc.) so that the back plane of the cassette holder is vertical. 2. Open the metal clasp of the beaded chain and attach the chain around the tubehead yoke where it connects with the X-ray arm (Figure 6).
Additional Notes 1. A second method for first-time attachment is outlined in Appendix C, VI. Image Geometry, C. Not centered within apparatus. 2. Retracting the clamp plates with black knobs will allow removal of the cone. 3. The cone will quickly realign into the adapter if the clamp plates with red knobs are not disturbed. These should remain in place for fast set-up.
B. Selecting the Correct Lead Aperture The lead aperture installed in your Accurad™200 headholder is designed to satisfactorily collimate the primary beam of all X-ray tubeheads utilizing the standard 8" technique. Two additional apertures have been included and are indicated for either 12" or 16" techniques and are so labeled. (To determine cone technique, measure from the focal point to the end of the X-ray cone.) When necessary, remove the two screws securing the lead aperture (lead disc with the square cut-out) (Figure 5) and install the correct aperture. Refer to Appendix
Figure 6 3. Lengthen the long support strap by sliding it through the plastic clasp. Engage the two plastic clasps (Figure 7). Adjust the long support strap to eliminate slack by pulling the free strap end through the clasp. 9
5. When not in use, the Accurad™-200 headholder may be removed and stored. Rest the cassette holder on a suitable support, disengage the two plastic clasps and leave the support chain and short strap around the tubehead yoke for simple reattachment of the unit. Retract the two black cone adapter knobs to remove the X-ray cone. 6. When the Accurad™-200 headholder is attached, the X-ray tubehead assembly may drift down prior to positioning on the patient. The X-ray arm may be counterbalanced, but it is not recommended. During the patient positioning procedure, the cassette holder is always supported by the patient regardless of drift. Patient support of the cassette holder reduces patient anxiety and increases control of the procedure.
Figure 7 4. With the Accurad™-200 headholder attached to the X-ray tubehead and supported by the support strap, the back plane of the cassette holder should be vertical and the upper rods of the Accurad™-200 headholder should be horizontal. Readjust the support strap if necessary. Note: Confirm that the cone is flush with the base of the lead cup (Figure 4).
10
III. Procedure for Use A. Loading the Cassette (Must be done in complete darkness or under the required filter.) 1. Remove the protective paper from the film cassette. 2. Open the cassette by releasing the 2 metal clasps (Figure 8).
Figure 9
B. Test Film Procedure Following the initial installation procedure, but prior to positioning the patient into the Accurad-200 headholder, confirm proper installation with a test film as follows: 1. Rest the cassette holder on a support (counter tip, chair arm rest, etc.) so the top of the cassette holder is horizontal, confirm that the cone is flush with the base of the lead cup. 2. Insert the loaded cassette into the cassette holder with the edge of the cassette flush with the edge of the cassette holder track. 3. Set the exposure timer at approximately 1⁄2 the suggested time for an adult male and make an exposure. 4. Process per instructions in Appendix B. 5. The resulting image should be approximately 13⁄4" – 2" with a 1⁄4" to 1⁄2" gray perimeter. The balance of the film should be window-pane clear. NOTE: If additional adjustment is required to center the cone, use the red and black knobs on the side of the cone adapter.
Figure 8 3. Insert the film into the cassette, close and latch. 4. Lanex Rare Earth screened cassettes: Film should not be stored in the cassette. The intensifying screens are coated with a protective layer which will wear away after prolonged cleaning. Only load the cassette prior to the radiographic procedure. 5. Use the color-coded indicator on the front of the cassette (Figure 9) to identify if your cassette is loaded or unloaded. (For example, the green dot may indicate that the cassette is unloaded, red loaded.) This indicator may also be used to identify if the film in the cassette is exposed or unexposed. To eliminate confusion, establish a procedure in your office for routine use of this indicator.
C. Test Film Troubleshooting Procedure 1. Problem: Balance of film not window-pane 11
clear. Solution: Film has been exposed to improper safelight illumination and/or white light leakage. Refer to Appendix B. 2. Problem: Image smaller than 13⁄4" square. Solution: Recheck tubehead specifications for 12" or 16" technique and install correct aperture. Refer to Appendix E. 3. Problem: Image 21 ⁄4" square resulting in image overlap. Solution: Recheck the tubehead specifications for 8" or 12" technique and install correct aperture. Refer to Appendix E. When you are satisfied with a proper test film as outlined above, proceed to patient set-up.
b. Set the ear plug on the modified twin axis adjustment wheel as recommended above and the pointer at 0 degrees. To move the ear plug, turn it one half turn to loosen, slide it to the desired position and tighten. To move the pointer, loosen the black knob, move it to the desired setting and tighten (Figure 11). Refer to Appendix D for procedure variations.
D. Patient Set-Up Protect the Patient from scatter or stray radiation with a lead apron. 1. To minimize slouching, seat the patient upright on a stool or in the dental chair with the head rest removed (Figure 10).
Figure 11 c. Have the patient position their right hand on their right shoulder, palm up. Have them take hold of the cassette holder (Figure 12).
Figure 10 2. When radiographing the right TMJ: a. Standard settings: The lead letter "R" must appear in the window. The modified twin axis wheel must be set at 0 degrees. A setting of 0 mm on the sliding scale will align the ear rods. If set between 7 and 12 mm, the patient will be angled slightly towards the cassette which may be more advantageous for radiographing the condyle.
Figure 12 d. As you guide the instrument into position, have the patient place the fixed ear rod projecting from the cassette holder into their right ear hole. (The fixed ear rod should be in the most posterior position on the cassette holder, with the "R" appearing over the window.) e. Guide the adjustable ear rod into the patient’s left ear hole (Figure 13). Important: Instruct 12
the patient to carefully insert the ear rod into the ear hole to its maximum position to obtain an optimal object-to-film relationship with minimal magnification and distortion. Appendix F contains more in-depth information on accurate head stabilization. f. Be sure the wheel remains horizontal. Secure in this position by tightening the silver knob (Figure 13). If the patient cannot close into maximum intercuspation at this point, back out the ear rod only to the point where they can comfortably achieve maximum intercuspation.
Figure 14b 2. Center the carriage over the patient’s head. Slide the nasion support rod through the carriage toward the patient (Figure 15).
Figure 15 3. The nasion piece must be brought into contact with the bridge of the nose (Figure 16) and support the head with the mandibular occlusal plane angled slightly down (5˚-7˚) (Figure 17) when the teeth are in maximum intercuspation.
Figure 13 g. Confirm that the patient’s mid-sagittal plane is vertical and the patient is sitting erect. Correct as necessary and recheck adjustments.
E. Adjusting the Nasion Aligner 1. Loosen the two black thumbscrews in the carriage on the horizontal rods (Figure 14a & b).
Figure 16
Figure 14a 13
1. Frankfort Plane external auditory meatus and lower rim of orbit or 2. Mandibular occlusal plane 5˚-7˚ Figure 17 4. Tighten the two carriage thumbscrews and the thumbscrew which secures the nasion height.
Figure 19
F. Recording Patient Positioning on the Film Envelope 1. On the patient film envelope (Figure 18), record the settings of the modified twin axis wheel. (See Appendix E for further instructions on ear rod placement.)
Figure 20
Figure 21 3. The radiographic position of the condyle is also recorded, as determined by the position of the mandible during the sequence of exposures (see Section III-G-3). 4. The developed film should be inserted into the patient’s film envelope and retained in the patient’s file after the radiographic procedure has been completed. The recorded data provides the necessary information to exactly duplicate the radiographic position for comparative viewing at a later time.
Figure 18 2. Record the three cranial alignments: (a) Horizontal – read scale from film transport to X-ray attachment (Figure 19), (b) AnteriorPosterior – read mid-sagittal scale from back to front of patient’s head (Figure 20), and (c) Vertical – read scale at nasion (Figure 21).
14
G. Exposing the Film 1. Your Accurad™-200 cassette contains Lanex Rare Earth intensifying screens. A compatible X-ray film such as Kodak® OG or T-mat G film should be used. 2. Although the enclosed suggested exposure guidelines are based on standards, it may be necessary to slightly alter them for your particular X-ray unit. Once these guidelines have been established and recorded on your exposure chart (refer to Section V) under "Selected Techniques," use becomes routine. For this reason, it is strongly recommended that a single "Scout" exposure be taken of one TMJ for the first few procedures prior to a full series to ensure proper patient positioning and darkroom technique. If the "Scout" film is acceptable, proceed with the rest of the series. If the film is unacceptable, refer to the troubleshooting schedule in Appendix C. 3. Three exposures may be taken on each side, with the mandible in varying positions. It is recommended that a preferred sequence of exposures be established so that your procedures are consistent and become standardized. The following is an example of this procedure: Exposure 1: Mandible in maximum intercupation (closed/clenched) Exposure 2: Mandible in rest position Exposure 3: Mandible opened to the maximum position Other exposures may be taken depending on patient treatment.
Figure 22 2. The first exposure is taken with the film cassette aligned flush to the edge of the cassette transport track in front of the patient (Figure 23).
Figure 23 3. For the second exposure, slide the film cassette in and align it between the two vertical edges of the cassette transport (in the middle of the transport) (Figure 24).
H. Radiographing the Temporomandibular Joint 1. Facing the patient, insert the cassette into the track of the cassette holder (Figure 22). The cassette should always be loaded from the front (the side by the patient’s face). The cassette label indicates cassette positioning for the appropriate side.
Figure 24
15
b. Adjustable Ear Rod: Loosen the black knob and move the pointer to the 180 degrees setting on the wheel and tighten. 8. Rotate the X-ray arm for exposure of the left TMJ. 9. Remove the nasion aligner and reinsert it into the opposite side. 10. Repeat parts D, E, F and G of Section III and steps 1-5 of Section H. (Be sure to invert the cassette before inserting it into the cassette holder so that the unexposed film is now in place behind the transport window and the cassette label indicates positioning for the left side.) 11. If necessary, readjust the nasion to support the head with the mandibular occlusal plane angled slightly down (5˚-7˚). 12. To remove the Accurad™-200 headholder form the X-ray tubehead, rest the cassette holder on a suitable support, disengage the two plastic clasps, loosen the two black clamp adjustment knobs (do not touch the red knobs) and remove.
4. For the third exposure, slide the cassette in until it is even with the far edge of the cassette transport track behind the patient’s ear (Figure 25).
Figure 25 5. After completing these three exposures of the TMJ, remove the film cassette. Loosen the carriage screws and slide the nasion away from the patient. Loosen the silver screw on the adjustable ear rod and retract it from the patient’s ear. 6. Lift the headholder away from the patient. Do not detach the Accurad™-200 from the cone. NOTE: Confirm that the cone is still flush with the base of the lead cup. 7. Change the settings to radiograph the left TMJ. (See page 12, D. Patient Positioning, 2. a.) a. Fixed Ear Rod: Turn the ear plug counterclockwise to loosen, slide it across the window so the "L" appears over the window, and tighten.
16
IV. Appendices Appendix A – Clinical Specifications
The following clinical specifications were determined by the research and clinical studies performed over a ten-year period by Dr. William Buhner* and several of his colleagues.
the condylar head and the roof of the glenoid fossa. • Differences in anatomical structures and their relationships may require a change of angulation in the vertical and/or horizontal planes to obtain the best view of the TMJ. This can be accomplished by adjusting the dial on the twin axis adjustment wheel per the instructions in Appendix D. Adherence to the standard technique (ear rod set at 0 or 180 degrees) should give satisfactory results in most instances. Refer to Appendix D for optional and corrected views. • Many find reference to the mandibular occlusal plane angle of a negative 5˚-7˚ affords them more consistent results than reference to the Frankfort plane due to misinterpretations of the Frankfort plane. * See Section VIII – Bibliography
• The 25-degree angulation of the central Xray beam of the Accurad™-200 was selected as an average for measuring, at the midpoint, the superior wall or roof of the glenoid fossa in relation to the Frankfort plane. This 25degree angulation is oriented to the roof of the glenoid fossa – not to the condylar head. The movable condylar head relates to the fixed glenoid fossa. • The correct angulation and exposure, both vertical and horizontal, will show a well defined line of bone density completely around the glenoid fossa from the articular tubercle to the petrotympanic fissure. The articular disk establishes the space between
Appendix B – Film Considerations
Extra-Oral Film Processing The quality of the radiograph will be affected by various light factors. The suggestions below are provided to help identify and correct these potential problems.
The Film The film used in conjunction with your Accurad™-200 is blue or green sensitive and is far more light sensitive than conventional intra-oral film. Screen film exposed to radiation is approximately eight times more sensitive to safelight illumination than unexposed film. Consequently, screen-exposed film should be processed promptly and the following criteria met.
Safelight – Filter must be a Type GBX with a 15 watt frosted light bulb. 6B, ML-1 or ML-2 filters with a 7 1/2 or 15 watt light bulb are unacceptable and will fog (darken) green-sensitive extraoral film. A GBX fluorescent dental safelight is recommended. All safelights must be mounted a minimum of 4 feet from the working surface. Manual Processing Use Kodak® GBX Developer and Fixer with an accurate darkroom thermometer immersed in the developer section. Do not agitate film during development. Process as indicated on the chart at the top of page 18. When scheduling solution changes, bear in mind that one 5" x 7" film contains more emulsion than 16 intra-orals and consequently will shorten the life of the solution. Maximum life is two weeks. Replenish 1 1/2 ounces of developer and fixer per film. Clean tanks with hot water. Do not use detergent.
The Darkroom Light-tight – Apply self-adhesive weatherstripping around all door, window or light fixtures which emit white light.
17
Temperature of Solution
Development Time Rinse Fix
60˚F (15.5˚C) 65˚F (18.5˚C) 68˚F (20.0˚C) 70˚F (21.0˚C)
8 1/2 minutes 6 minutes 5 minutes 4 1/2 minutes
30 seconds 30 seconds 30 seconds 30 seconds
Automatic Processing A 5-minute dry to dry cycle is recommended. Confirm manufacturer’s recommended developer temperature with accurate thermometer. For optimum results, use Kodak® Readymatic premixed solution #102-8869.
4 minutes 4 minutes 4 minutes 4 minutes
Final Wash in Running Water 20 minutes 20 minutes 20 minutes 20 minutes
Film/Screen Combinations With Lanex Rare Earth Intensifying Screens use only Kodak® 5" x 7" OG green-sensitive film.
18
Appendix C – Accurad™-200 Headholder Troubleshooting Schedule
V. Artifacts A. Scratches attributed to transport rollers or handling. B. Fingerprints. C. Fingernail indents. D. Ear ring image. E. Fixer stains. F. Smears (debris on transport rollers). G. Other:
The following schedule has been prepared to help you achieve the highest quality radiographic results possible. When evaluating your processed films, check the appropriate boxes to highlight the apparent problems seen on your films and identify their probable causes. I.
Insufficient development (due to improper solutions, time/temperature imbalance, etc.) A. Excessive hypo (results in excessive matte finish, wavy patterns along film edge – visible by reflecting overhead light off film surface). B. Graininess.
VI. Image geometry A. Too large (results in unnecessary scatter and patient radiation, further sensitizes unexposed film area). Use next smaller lead aperture. B. Too small (insufficient to record required anatomy). Use next larger lead aperture. C. Cone not centered within adapter. To adjust, remove cone from the X-ray machine. Back out the red and black screws on the Accurad-200 cone adapter. Insert the X-ray cone into the adapter until the cone abuts uniformly against the lead cup. Tighten both the red and black screws (lightly to moderately) and center the X-ray cone within the adapter. Secure the red screws with lock nuts. Remove the X-ray cone and install onto the tubehead. Attach the Accurad-200 by inserting the cone into the adapter until it mates flush with the base of the lead cup and rests against the two preset clamp plates. While maintaining these contacts, turn the black knobs until the cone is securely held by the clamps. Visually confirm that the X-ray cone is centered. Readjust if necessary. Uniform tightening will reduce alignment error. D. Not symmetrical (See "C" above). E. Lead letters not positioned in primary image. Move ear positioner slide until the lead letter is positioned in the window.
II. Fog A. Light fog (due to white light leaks, improper safelight). B. Chemical fog (due to wrong/aged/ contaminated solutions). III. Adjustable ear rod not inserted into its maximum. Results in: A. Fossae appear high within image. Should be centered approximately. B. Fossae outline acceptable. Condyle outline in centric occlusion and rest positions unacceptable. C. Excessive discrepancy between nasion aligner settings. (Should be identical if patient positions the adjustable ear rod into its maximum.) IV. Blurred image. Suspect one or more of the following: A. Fog B. Adjustable ear rod not inserted into its maximum C. Adjustable ear rod not horizontal in respective position. D. Insufficient development. E. Insufficient rinse. F. Insufficient exposure time. G. Excessive exposure time. H. Angle of patient’s mandibular occlusal plane incorrect (should be positioned down 5 to 7 degrees). Angled too far down Angled too far up I. Patient characteristics
VII. Rare Earth Intensifying Screens Lanex Film type Other A. Quantum Mottle Excessive Acceptable Similar to grain in appearance but a product of film processing. 19
Appendix D – Procedure Variations
When you have determined other view(s) you would like to see on your radiographs and what angulation you will need to achieve these views, follow this procedure:
graph the left condyle on a patient with 90 mm inter-ear distance at 15 degree horizontal and 20 degree vertical angles, you would set the pointer at 143 degrees and the ear plug at 26 mm. c. Corrected Transcranial (using the submental vertex radiograph). Using the appropriate chart, use the horizontal angle derived from the submental vertex radiograph and move down the column until you reach the row for your desired vertical angle. Example: To radiograph the left condyle on a patient with 120 mm inter-ear distance at a 25 degree horizontal and the standard 25 degree vertical angles, you would set the pointer at 180 degrees and the ear plug at 51 mm. Following this procedure, you will achieve a corrected transcranial on the Accurad-200. d. Make a series of exposures as outlined on pages 14-16. By using the settings on the modified twin axis adjustment wheel as described on the charts, your radiographs will provide repeatable, quantifiable data for use in progressive treatment.
I. Determine the inter-ear distance of the patient by reading the calibrated scale on the long rod on the wheel. II. Use the following charts as guidelines to enable you to set the horizontal and vertical angles of the wheel. These charts are for 90 mm, 120 mm, 150 mm and 180 mm inter-ear distance. Use the chart which is closest to the patient’s measurement. III. Three variations can be achieved: a. Standard. This procedure is described on pages 12 & 13 under D. Patient Set-Up. It is based upon using the 0 degree horizontal and 25 degree vertical standard settings which are the same on all charts. b. Modified. Using the appropriate chart, select the horizontal angle desired and move down that column until you reach the row for your desired vertical angle. The top number in each box (measured in degrees) corresponds to the setting of the pointer on the wheel. Example: To radio-
Sample
Left Condyle 90mm
Horizontal Angle Desired (From Submental Vertex)
Vertical Angle Desired
Pointer reading form twin axis wheel Reading from sliding ear plug on twin axis wheel
Intercondylar distance
0˚
5˚
10˚
15˚
20˚
25˚
30˚
15˚
51˚ 33mm
72˚ 29mm
100˚ 29mm
123˚ 31mm
138˚ 36mm
148˚ 42mm
154˚ 48mm
20˚
32˚ 28mm
58˚ 22mm
110˚ 21mm
143˚ 26mm
157˚ 32mm
163˚ 39mm
166˚ 46mm
25˚ Standard
180˚ 0mm
180˚ 8mm
180˚ 16mm
180˚ 23mm
180˚ 31mm
180˚ 38mm
180˚ 45mm
30˚
328˚ 28mm
302˚ 22mm
250˚ 21mm
217˚ 26mm
203˚ 32mm
197˚ 39mm
194˚ 46mm
35˚
309˚ 33mm
288˚ 29mm
260˚ 29mm
237˚ 31mm
222˚ 36mm
212˚ 42mm
206˚ 48mm
20
Left Condyle 90mm
Horizontal Angle Desired (From Submental Vertex) 0˚
5˚
10˚
15˚
20˚
25˚
30˚
15˚
51˚ 33mm
72˚ 29mm
100˚ 29mm
123˚ 31mm
138˚ 36mm
148˚ 42mm
154˚ 48mm
20˚
32˚ 28mm
58˚ 22mm
110˚ 21mm
143˚ 26mm
157˚ 32mm
163˚ 39mm
166˚ 46mm
180˚ 0mm
180˚ 8mm
180˚ 16mm
180˚ 23mm
180˚ 31mm
180˚ 38mm
180˚ 45mm
30˚
328˚ 28mm
302˚ 22mm
250˚ 21mm
217˚ 26mm
203˚ 32mm
197˚ 39mm
194˚ 46mm
35˚
309˚ 33mm
288˚ 29mm
260˚ 29mm
237˚ 31mm
222˚ 36mm
212˚ 42mm
206˚ 48mm
Vertical Angle Desired
25˚ Standard
Right Condyle 90mm
Horizontal Angle Desired (From Submental Vertex) 0˚
5˚
10˚
15˚
20˚
25˚
30˚
15˚
129˚ 33mm
108˚ 29mm
80˚ 29mm
57˚ 31mm
42˚ 36mm
32˚ 42mm
26˚ 48mm
20˚
148˚ 28mm
122˚ 22mm
70˚ 21mm
37˚ 26mm
23˚ 32mm
17˚ 39mm
14˚ 46mm
180˚ 0mm
180˚ 8mm
180˚ 16mm
180˚ 23mm
180˚ 31mm
180˚ 38mm
180˚ 45mm
30˚
212˚ 28mm
238˚ 22mm
290˚ 21mm
323˚ 26mm
337˚ 32mm
343˚ 39mm
346˚ 46mm
35˚
231˚ 33mm
252˚ 29mm
280˚ 29mm
303˚ 31mm
318˚ 36mm
328˚ 42mm
334˚ 48mm
Vertical Angle Desired
25˚ Standard
21